
TL;DR: About 10% of newborns need some help to start breathing at birth, and roughly 1% need extensive resuscitation. The NRP algorithm is the step-by-step roadmap that guides L&D and NICU teams through those first critical minutes. Here’s a plain-language walkthrough from initial steps to chest compressions to epinephrine for nurses certifying or renewing in Houston.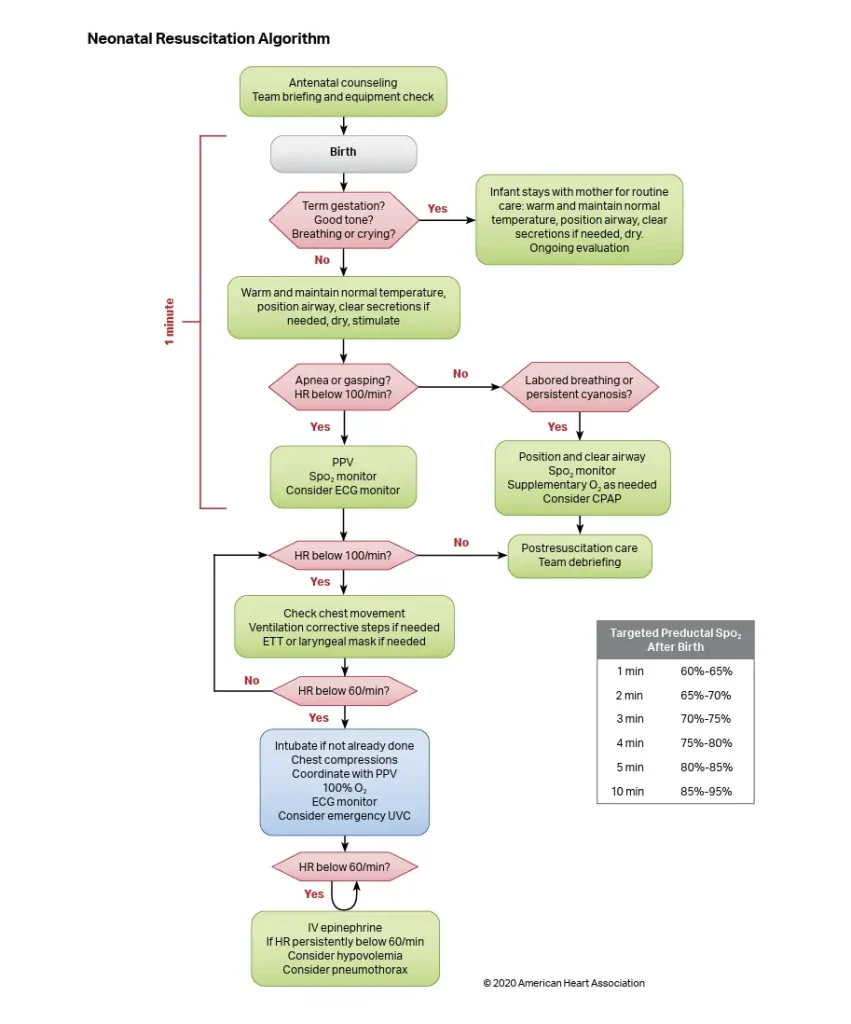
What is the NRP algorithm?
The NRP algorithm is the standardized decision tree used in U.S. delivery rooms to evaluate and resuscitate newborns who are not breathing effectively at birth.
It is published by the American Academy of Pediatrics and the American Heart Association as part of the Neonatal Resuscitation Program and is the foundation of every NRP class.
If you are studying the NRP algorithm 8th Edition or preparing for the upcoming 9th Edition, the structure remains familiar:
- Rapid assessment
- Ventilation first
- Reassessment
- Escalation only if ventilation is not enough
- Chest compressions when the heart rate remains below the threshold
- Epinephrine when compressions and ventilation do not restore heart rate
Recommended internal link:
Click here to read about our Neonatal Resuscitation Program in Houston
The Golden Minute: your first 60 seconds
The Golden Minute is the single most important concept in NRP.
From the moment a baby is born, the team has approximately 60 seconds to:
- Complete the initial steps.
- Reassess breathing and heart rate.
- Begin positive pressure ventilation, or PPV, if the baby is apneic, gasping, or has a heart rate below 100 bpm.
If effective ventilation is not established within that first minute, outcomes can worsen. That is why NRP team prep, equipment checks, role assignment, and communication happen before the baby is born.
Step-by-step walkthrough of the NRP algorithm
The NRP algorithm follows a structured clinical sequence. The goal is to make the right decision quickly, especially when the newborn is not transitioning well after delivery.
1. Rapid evaluation at birth
At birth, the team asks three questions at the same time:
- Is the baby term?
- Does the baby have good muscle tone?
- Is the baby breathing or crying?
If the answer is yes to all three, the baby can usually receive routine care with the mother.
If the answer is no to any of these questions, the baby should move to the warmer for further assessment and intervention.
2. Initial steps in the first 30 seconds
The initial steps are designed to support breathing, warmth, and airway positioning.
These steps include:
- Provide warmth with a radiant warmer.
- Use plastic wrap for preterm infants under 32 weeks when appropriate.
- Position the airway in the sniffing position.
- Clear secretions only if the airway is obstructed.
- Suction the mouth, then the nose, when needed.
- Dry and stimulate the newborn.
3. Assess heart rate and breathing
After the initial steps, reassess the baby’s heart rate and breathing.
Use this decision path:
- Heart rate 100 or higher and breathing well: routine care and observation.
- Heart rate 100 or higher with labored breathing or persistent cyanosis: SpO₂ monitoring and consider CPAP.
- Heart rate below 100, apnea, or gasping: start positive pressure ventilation.
4. Start positive pressure ventilation
Positive pressure ventilation is the priority intervention in most neonatal resuscitation.
Effective PPV should be delivered at 40 to 60 breaths per minute while watching for:
- Visible chest rise
- Improving heart rate
- Better color
- Better oxygen saturation over time
- Improved respiratory effort
Most newborn resuscitations succeed at this step when ventilation is effective.

5. Use MR. SOPA when ventilation is not effective
If the heart rate is not improving or the chest is not rising, run through the MR. SOPA corrective steps.
MR. SOPA stands for:
- M: Mask adjustment
- R: Reposition the head
- S: Suction mouth and nose
- O: Open the mouth
- P: Increase pressure
- A: Consider alternative airway, such as LMA or ETT
Most “failed PPV” situations are actually mask seal or head position problems. These can often be corrected in seconds.
6. Begin chest compressions if heart rate remains below 60
Chest compressions are only indicated if the heart rate remains below 60 bpm after 30 seconds of effective ventilation.
When compressions are needed:
- Ratio: 3 compressions to 1 ventilation
- Rate: 90 compressions and 30 ventilations per minute
- Total events: 120 events per minute
- Depth: one-third the anterior-posterior diameter of the chest
- Preferred technique: two-thumb encircling-hands method
In neonatal resuscitation, compressions do not replace ventilation. They work with ventilation because most newborn emergencies are respiratory first.
7. Give epinephrine if heart rate remains below 60
If the heart rate remains below 60 after 60 seconds of coordinated compressions and ventilation, epinephrine is indicated.
Standard epinephrine guidance includes:
- IV/IO dose: 0.02 mg/kg
- Dose range: 0.01 to 0.03 mg/kg
- Concentration: 0.1 mg/mL
- Preferred route: IV or intraosseous
- ETT route: only if vascular access is delayed
- Repeat timing: every 3 to 5 minutes as needed
8. Consider volume expansion if hypovolemia is suspected
Volume expansion may be considered if there is evidence of blood loss or poor perfusion that is not responding to other interventions.
Common guidance includes:
- Normal saline
- 10 mL/kg
- Given over 5 to 10 minutes
- IV or IO route
This step is not automatic. It depends on clinical signs and the resuscitation context.
FAQ: Common NRP algorithm questions
How long do we continue resuscitation?
Per AHA/AAP guidance, continued resuscitation may be reasonable while reversible causes are being addressed. Discussion about discontinuation is reasonable around 20 minutes of asystole.
Always follow your facility’s protocols and current medical direction.
What if we do not have IV access?
The team should establish umbilical venous access or use intraosseous access when needed.
ETT epinephrine is a last-line route if vascular access is delayed and uses a different dose range, often 0.05 to 0.1 mg/kg.
Do we need an advanced airway right away?
No. Effective bag-mask ventilation handles most cases.
Advanced airway placement may be considered if:
- PPV is prolonged
- MR. SOPA does not correct ventilation
- Chest compressions are needed
- The team cannot achieve effective ventilation with the bag-mask technique
How to learn the NRP algorithm in Houston
Reading the algorithm is the easy part. Performing it as a team in real time is where NRP training becomes valuable.
During an in-person skills session, you practice:
- Equipment setup
- Team role assignment
- Bag-mask ventilation
- MR. SOPA corrective steps
- Chest compressions
- Megacode scenarios
- Communication under pressure
- Real-time decision-making
Health Street CPRologist runs in-person NRP skills sessions in West Houston. You complete the online modules through the NRP Learning Platform first, then come in for hands-on simulation with mannequins, real bag-mask devices, and team-based megacode practice.
Find the next NRP certification class in Houston
Health Street CPRologist offers NRP certification classes for healthcare professionals in Houston, including L&D nurses, NICU nurses, respiratory therapists, and hospital-based clinical teams.
Register Here By Clicking The Button
Review and educational note

Reviewed by: Leah F., Operations Director, Health Street CPRologist.
This content is educational only. Follow your facility’s protocols and current AHA/AAP guidelines. Confirm your required class type with your employer, licensing body, hospital educator, or academic program before registration.


